Diseases caused by bacteria
with special reference to antibiotic resistance
Staphylococcus aureus ... Streptococcus pneumoniae ... Klebsiella pneumoniae ... Escherichia coli (E. coli) ...
Enterococcus spp. .. Pseudomonas aeruginosa .. Clostridium difficile ...
Enterococcus spp. .. Pseudomonas aeruginosa .. Clostridium difficile ...
For each organism, I have presented some information about its microscopic appearance and its characteristics in culture, together with background information - emphasising that even pathogenic bacteria have another side to them, some details of the diseases caused by these bacteria, and the modern problems caused as a result of the development of resistance to antibiotics.
Staphylococcus aureus
- sometimes called golden staph
Image courtesy CDC/ Matthew J. Arduino, DRPH
This is a false colour scanning electron micrograph. Some of the cells can be seen to be preparing to divide. Staphylococci tend to cling together after dividing in different directions and so resemble a bunch of grapes. | To a bacteriologist,Staphylococcus aureus is afacultatively anaerobic Gram-positive coccus. When cultured on blood agar it exhibits haemolysis and it testscoagulase-positive and catalase-positive. |  haemolysis")
Image courtesy The Royal Veterinary and Agricultural University of Copenhagen
On this blood agar plate Staphylococcus aureuscolonies show whitish grey and glistening. Mouseover to see zones of haemolysis, visible when lit from below. |
Background information
Staphylococcus aureus is part of normal skin flora (possibly including nasal passages) in a large proportion of the human population, without causing problems to the carrier.It may be passed from person to person by direct contact or via surfaces, including door handles. It has been shown to persist on hospital privacy curtains. This underlines the importance of hand-washing and hygiene.
It may cause disease if it enters an open wound and it can become a major problem for people with damaged or depressed immune systems, either from chronic disease, such as HIV, or in those undergoing chemotherapy, which represses the activity of the immune system.
The related species Staphylococcus epidermidis (used to be known as S. albus) also exists on skin and may play a protective role against S. aureus in normal conditions.
Causes (disease):
| Staphylococcus aureus may cause minor skin infections such as pimples and boils, but these may become deep-seated, causing abscesses etc. If it enters the blood it can cause a number of problems in the body: bacteremia and sepsis, toxic shock syndrome (TSS), pneumonia, meningitis, osteomyelitis, endocarditis. Some strains produce (entero)toxins which can cause food poisoning. Staphylococcus aureus is likely to cause problems in hospital patients:
| 
Image courtesy CDC/ Bruno Coignard, M.D.; Jeff Hageman, M.H.S.
This is a cutaneous (skin) abscess on the hip of a prison inmate, spontaneously releasing its contents as pus. |
Resistance Problems
 Before antibiotics were discovered, Staphylococcus aureus infections were frequently fatal. Originally Staphylococcus aureus bacteria were easily killed by penicillin, as shown by the zone of inhibition on this Petri dish from Alexander Fleming in 1928.
Before antibiotics were discovered, Staphylococcus aureus infections were frequently fatal. Originally Staphylococcus aureus bacteria were easily killed by penicillin, as shown by the zone of inhibition on this Petri dish from Alexander Fleming in 1928.Some bacteria by chance acquired the ability to break down and inactivate penicillin, using the enzyme penicillinase, which breaks open the beta lactam ring. Since these penicillin-resistant strains were not killed by it, they reproduced and replaced the original (penicillin sensitive) strains of Staphylococcus aureus. These are not necessarily more aggressive pathogens, but more difficult to control.
By the end of the 1950's penicillin resistance was a major problem,and spreading round the world. Several derivative compounds were developed for medicinal use, and categorised as beta lactamase sensitive or insensitive, depending on bacterial resistance to them.
Methicillin was developed in the early 1960's, and fell into the beta lactamase insensitive category. It is no longer produced - having been displaced by flucloxacillin, and dicloxacillin - but it gives its name (or at least its initial) to one of the most well known "superbugs".
The main current cause for concern is MRSA, a methicillin-resistant form of Staphylococcus aureus.
There is some variation in abundance and virulence of MRSA from country to country, as well as between community and hospital strains.
It is also likely to be resistant to basic penicillin and more recently developed forms.
Other antibiotics, e.g. vancomycin, teicoplanin or linezolid, may be used to treat MRSA, but they need to be (a) injected, either directly into a vein or fed into the blood stream via a drip rather than by mouth and (b) given at quite a high dose. Treatment is likely to involve several weeks in hospital.
Streptococcus pneumoniae
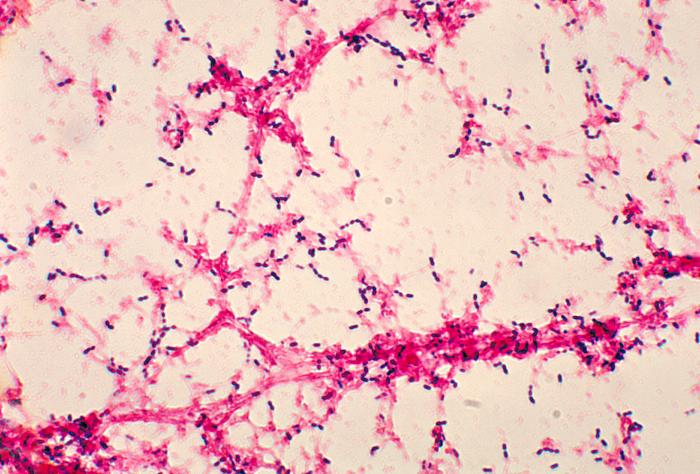
Image courtesy CDC/Dr. Mike Miller
This is a photomicrograph of Streptococcus pneumoniaebacteria, grown in a liquid medium containing blood. It is a gram-stained preparation, seen using a light microscope. The bacteria can be seen as purple dots in short rows, and the pinkish strands are fibres of fibrin in the clotted blood. | Initially this organism was known as Pneumococcus, then renamed Diplococcus pneumoniae because it was commonly seen as pairs of cells in sputum from people infected with pneumonia. When grown in liquid media in the lab it forms chains so it is now known asStreptococcus pneumoniae. It was first isolated and described on 1881, by two pioneers of bacteriology working independently of one another: Louis Pasteur in France and George Miller Sternberg in America.
This organism was used to show the significance of DNA as the carrier of genetic information when the 'transforming principle' passed from a virulent but killed strain of bacteria (a 'smooth' form, with a capsule) to a non-virulent strain (a 'rough' form, with no capsule), as shown by experiments on mice. This transformation, discovered by Frederick Griffith in 1928, was proved in 1944 by Oswald Avery, Colin MacLeod, and Maclyn McCarty to be caused by DNA not protein.
|  Streptococcus pneumoniae is a gram-positive, catalase-negative coccus. It is said to be an aerotolerant anaerobe. When grown on agar containing blood it shows alpha haemolysis. |
Background information
Streptococcus pneumoniae is very common and may be found in the back of the nose and throat, or the upper respiratory tract. Up to 40% of healthy adults and children show no adverse effects.Causes (disease):
Streptococcus pneumoniae can be one cause of lobar pneumonia (infection of the lung), especially in young adults. It is estimated that 25% of all community-acquired pneumonia is due to this species.Other forms of pneumonia may be caused by different bacteria including Staphylococcus, Pseudomonas, Haemophilus, Chlamydia and Mycoplasma, or by certain viruses, fungi or protozoans.
Streptococcus pneumoniae may also cause infections of the sinuses or ears. As a result, it may go on to cause bacterial meningitis. It may also infect bones andjoints as well as internal organs, especially in children and elderly people.
It has quite a complex cell wall which tends to become attached to human cells, and produces several toxins which perforate cell membranes and cause tissue damage. There are many possible proteins in the bacterial cell wall and membrane, and abot 90 different strains or serotypes can be identified, allowing the monitoring of outbreaks but a mixed vaccine must be developed to deal with the most likely strains.
Some strains have a capsule which makes them more virulent, and some have pili (hair-like structures that extend from the surface) which assist in the colonization of the upper respiratory tract. They also increase the formation of cytokines - signalling compounds produced by the immune system, and this causes tissue breakdown and allows invasive infection.
Resistance Problems
S. pneumoniae has a natural transformation system as a mechanism for genetic exchange (horizontal gene transfer) with related and unrelated species. It has been shown that genes coding for alterations in penicillin binding proteins have been passed in this way so that resistance to beta lactam antibiotics has quickly spread in the last 20 years.As it grows in numbers quite fast and achieves large populations when it causes infections, it achieves conditions which quickly lead to random mutations, the most advantageous of which are selected for and consequently get to dominate the population.
Multiple antibiotic resistance now covers the globe and has rapidly increased since 1995.
Klebsiella pneumoniae

Klebsiella spp. as seen under the light microscope
| Klebsiella species are nonmotile, rod-shaped,gram-negative, catalase-positive, oxidase-negative, lactose fermenting, facultatively anaerobic bacteria with a prominent polysaccharide capsule. The genus Klebsiella is named after Theodor Albrecht Edwin Klebs, a German-Swiss pathologist and microbiologist who identified the bacterium causing diphtheria. |  Klebsiella pneumoniae ferments lactose and produces pink colonies on McConkey agar. The shiny (mucoid) colonies indicate the presence of the capsule. |
Background
K. pneumoniae is part of normal skin, mouth and gut flora - no problem to most healthy people.Causes (disease)
When K. pneumoniae colonises the respiratory system it can cause bronchopneumonia or bronchial pneumonia - as distinct from lobar pneumonia (see above). This results in the acute inflammation of the walls of the bronchioles (small air passages leading from the windpipe and bronchi towards the alveoli: the terminal air sacs) and consequent congestion with pus. Usually there are several sites of infection, on both lungs.Endotracheal intubation (insertion of a tube into the windpipe to assist breathing) sometimes results in this infection.
Bronchopneumonia may also be caused by Staphylococcus aureus, E. coli, and Pseudomonas.
Klebsiella pneumoniae can also cause urinary tract infections often associated with catheters (UTIs) as well as infecting surgical wound sites.
Resistance problems
In healthcare settings, Klebsiella infections commonly occur among sick patients who are receiving treatment for other conditions, especially those with a weakened immune system or on long courses of certain antibiotics. Patients on ventilators (breathing machines) or intravenous (vein) catheters, and urinary catheters are most at risk for Klebsiella infections.Some Klebsiella strains have become highly resistant to antibiotics, especially carbapenems which are the last line of defence against Gram-negative infections
Escherichia coli (E. coli)

Enteropathogenic strain (colourized scanning electron micrograph)") Image courtesy CDC/ National Escherichia, Shigella, Vibrio Reference Unit at CDC This is a colourized scanning electron micrograph (SEM) depicting a number of Gram-negative Escherichia coli bacteria of the strain O157:H7. |  Escherichia coli as seen under the light microscope |
In the past it has been called Bacterium coli and Bacillus coli, but it was (re-)named after Theodor Escherich, a leading German bacteriologist in the field of paediatrics, who first described it in 1886. The specific part of the binomial name "coli" means " of the colon" - the large intestine (also known as the bowel).
It has been widely used in laboratories for over 60 years because it is easy to grow and offers little danger of infection, and it has been extensively used in virology and recombinant DNA work.
As it leaves the body in faeces and can survive for some time afterwards, it serves as an indicator of faecal contamination of the environment and foods. A number of microbiological test procedures have been developed for this purpose. It lends itself to tests involving selective media based on recreating conditions within the colon.
It is a Gram-negative, facultatively anaerobic, rod-shaped bacterium. It is non-sporulating i.e. it does not produce spores.
Some strains are motile i.e they possess flagella, which are described as peritrichous i.e. projecting outwards all round the surface of the cell wall.
Background information
There are many strains of E. coli.The harmless strains are part of the normal flora of the gut. It is said that they are beneficial in that they produce vitamin K2, and that they prevent the establishment of pathogenic bacteria within the intestine - an effect that may be counteracted if antibiotics are used for treating other bacterial conditions.
Interestingly, E. coli is one of the first bacteria to colonise the gut of new-born children, but not those born by Caesarean section.
Disease caused by E. coli
Enteropathogenic forms of E.coli have recently become more well known than the "ordinary" forms. These cause severe stomach cramps, diarrhoea (often bloody), and vomiting and perhaps slight fever. They produce a toxin that can attack the body in several areas: the gut (causing bloody diarrhoea), the kidneys (causing kidney failure), and sometimes the nervous system.One strain in particular (known as O157, O157 H7, STEC, VTEC or EHEC) has been responsible for most problems i.e outbreaks of “E. coli” infections around the world, first noted in 1982. In addition, other kinds of E. coli (called serogroups) can cause disease of varying seriousness. These serotypes are based on antigensassociated with various components: (O: outer cell wall layer, H: flagellin, K: capsule).
A recent outbreak in Germany was caused by a strain now known as O104:H4 from contaminated seed sprouts.
The faecal-oral transmission route is the main way in which pathogenic strains of the bacterium cause disease.
Many incidences of holiday diarrhoea have been attributed to it, especially after consuming food which has been contaminated with faeces, either in preparation following poor lavatory hygiene or as a result of the application of (animal or other) manure to land on which crops are grown. Salads are especially suspect in this respect. Unpasteurized (raw) milk, soft cheeses made from raw milk and undercooked beefburgers are common sources of infection, as well as swallowing lake water while swimming, visiting petting zoos and other animal exhibits.
Resistance problems
Digestive system infections are not treated with antibiotics; recent strains e.g O104:H4 are resistant to most antibiotics. This is likely to be due to previous "environmental" exposure to them.Infections within other areas of the body can cause a variety of problems:
- urinary tract infections (UTIs), which may lead to:
- bacteremia (presence of bacteria in the blood - not quite the same as "blood poisoning")
- E. coli pneumonia (bronchopneumonia of the lower lobes) - especially in patients weakened by other conditions e.g. diabetes mellitus, alcoholism, chronic obstructive pulmonary disease
- cholecystitis - inflammation of the gallbladder
- acute bacterial meningitis in newborn children (may also be caused by group B streptococcal infections)
- this may lead to:
Some strains possess P fimbriae (many short proteinaceous appendages) that are used to adhere to human body cells, especially epithelial cells of the urinary tract.
Trimethoprim is the drug of first choice for the treatment of uncomplicated urinary tract infections although 10-20% of E. coli infections will be resistant to it. Other antibiotics which may be used as first-line agents if a patient is allergic to trimethoprim include nitrofurantoin and cefalexin. Amoxicillin is not used routinely as 50% of organisms will be resistant to it.
Enterococcus spp.

Image courtesy CDC/ Janice Haney Carr
This is a monochrome (uncoloured) scanning electromicrograph. | Enterococci are facultatively anaerobic Gram-positive cocci. In culture media they do not show haemolysis. The most clinically relevant of these bacteria are E. faecalis and E. faecium. The term enterococci may be used in a general sense to mean round-shaped bacteria (cocci) found in the gut, but if used as a Genus (Enterococcus spp.), it should be italicised. They were previously categorised as "Group D" Streptococcus organisms. |
Background information
Enterococcus spp. are said to be commensal, inhabiting the gastrointestinal tracts of humans. As such, they are not a problem unless complications arise following surgery or deterioration in health.Disease caused by Enterococcus spp.
Enterococcus spp. from a patient's intestine can spread to other parts of the body, often causing urinary tract infection, infection within the abdomen, and infection of operational wound sites. From here it can spread and cause infections in a number of areas such as endocarditis.Antibiotic Resistance problems
Enterococci from the gut are commonly found to have resistance to a variety of antibiotics and thus treatment of supplementary infections in the hospital setting presents a challenge.The current focus of attention is on vancomycin-resistant Enterococci (VRE).
A number of resistance genes are known; these are carried on plasmids or transposons.
Pseudomonas aeruginosa

Image courtesy CDC/ Janice Haney Carr
This is another false colour scanning electron micrograph. | Pseudomonas aeruginosa - also known as Pseudomonas pyocyanea - is a Gram-negative, aerobic orfacultatively anaerobic, rod-shaped bacterium. It is motile. When grown on certain types of agar in the laboratory, it produces green pigments. The genus name Pseudomonas means 'false unit', although it might be an attempt to distinguish it from another organism living in water, probably a protoctistan. The species name aeruginosa refers to the blue-green pigment produced in culture. |
Background information
Pseudomonas aeruginosa is widely distributed in the environment - in soil and water, especially stagnant water. It may be found on the surface of human skin and may be said to be part of the normal skin flora for some people.Because it is quite flexible in its nutrition and respiration, it can colonise many areas around the home and hospital, and (non-sterile areas) inside the human body. This is seen as less of a problem than growth of P. aeruginosa in normally sterile areas.
Disease caused by Pseudomonas aeruginosa
Under some circumstances Pseudomonas aeruginosa may cause infections in the body. It may be considered as an opportunistic, nosocomial pathogen of immunocompromised individuals, including premature and newly-born babies.These infections commonly involve the pulmonary tract, urinary tract infections, burns, wounds, and other blood infections
It also commonly affects those with the condition cystic fibrosis, in which thick mucus in the lungs restricts diffusion of oxygen, providing conditions which favour its growth.
P. aeruginosa may also cause Hot tub folliculitis - a skin rash caused by bacterial growth in hair follicles, when hygiene falls due to inadequate treatment of water in these environments, and it has also been implicated in osteomyelitis due to puncture wounds of the foot, resulting in direct inoculation with P. aeruginosa via the foam padding found in tennis shoes.
Antibiotic resistance problems
Pseudomonas aeruginosa is not easily controlled by antibiotics, because it is Gram-negative and has a fairly impermeable outer layer (envelope) and it can also turn on "pumps" that remove antibiotics from the cell.Additionally, it may benefit both physically and geneticaly from the formation of biofilms within the body.
P. aeruginosa is generally controllable by the use of certain antibiotics, although the classically-used examples are ineffective.
The Health Protection Agency suggests the use of third generation cephalosporins (ceftazidime), carbapenems (imipenem and meropenem), aminoglycosides (gentamicin and tobramycin) and colistin. For serious infections, broad-spectrum penicillins are recommended in combination with an aminoglycoside.
Clostridium difficile

Image courtesy CDC/ Lois S. Wiggs & Janice Carr
| Clostridium difficile is a Gram-positive, anaerobic spore-forming rod-shaped bacterium.
Its specific name (difficile) - meaning difficult - may be pronounced in a number of ways, depending on different styles of Latin or even French.
Being anaerobic spore-formers, Clostridium species are in a category of their own. They also produce toxins which have adverse effects on the human body. Other members of the genusClostridium cause tetanus (jockjaw), botulism, and gangrene.
Most bacteria form only vegetative cells, and although they grow quickly and can cause different sorts of problems inside the body, outside the body they are easily killed by exposure to reasonably high temperature, dry conditions, and certain sorts of chemicals - antiseptics and disinfectants. The spores formed by Clostridium species are extremely resistant to these conditions, and remain viable for months or years. In fact these spores can withstand exposure to high temperatures and strong disinfectant chemicals. As anaerobic organisms, they can cause problems within the body as they can respire, function and reproduce in parts of the body that are not well supplied with oxygen, such as in the gut or deep within muscles. |
Background information
Clostridium difficile bacteria are naturally found in the gut of some people, probably kept under control by the activities of other harmless bacteria there - it may be called commensal. Some cells of Clostridium difficile are transformed into spores, which will leave the body in faeces and on underclothes and bedclothes, but presumably these do not cause any further problems for these people. The spores of C. difficile can survive in the environment in a state of suspended animation for months or years.Disease caused by Clostridium difficile
In the hospital or other healthcare environment spores may be spread from one patient to another, perhaps when bedclothes are changed. Spores of Clostridium difficile entering the body can germinate and the resulting vegetative bacterial cells can grow in number. This may cause flu-like symptoms or (mild?) colitis.
However, if antibiotics are administered, they may eliminate other competing micro-organisms in the gut, causing unchecked growth of C. difficile. In this context cephalosporins and in particular quinolones and clindamycin are considered to be high risk antibiotics.
Growth of C. difficile may cause more severe diarrhoea - the condition being known as antibiotic-associated diarrhoea (AAD). Toxins from C. difficile can cause severe inflammation of the colon - pseudomembranous colitis may result. This may be treated using completely different antibiotics.
Growth of C. difficile may cause more severe diarrhoea - the condition being known as antibiotic-associated diarrhoea (AAD). Toxins from C. difficile can cause severe inflammation of the colon - pseudomembranous colitis may result. This may be treated using completely different antibiotics.

















